ABDM Integration Explained: ABHA, HIE/CM, HFR, HPR for Developers
If you're building healthcare software for Indian users, the Ayushman Bharat Digital Mission is now the central interoperability spine you need to plug into. There is decent documentation, but it's scattered, regulator-toned, and missing the developer's perspective. This is the developer's view.
Key takeaways
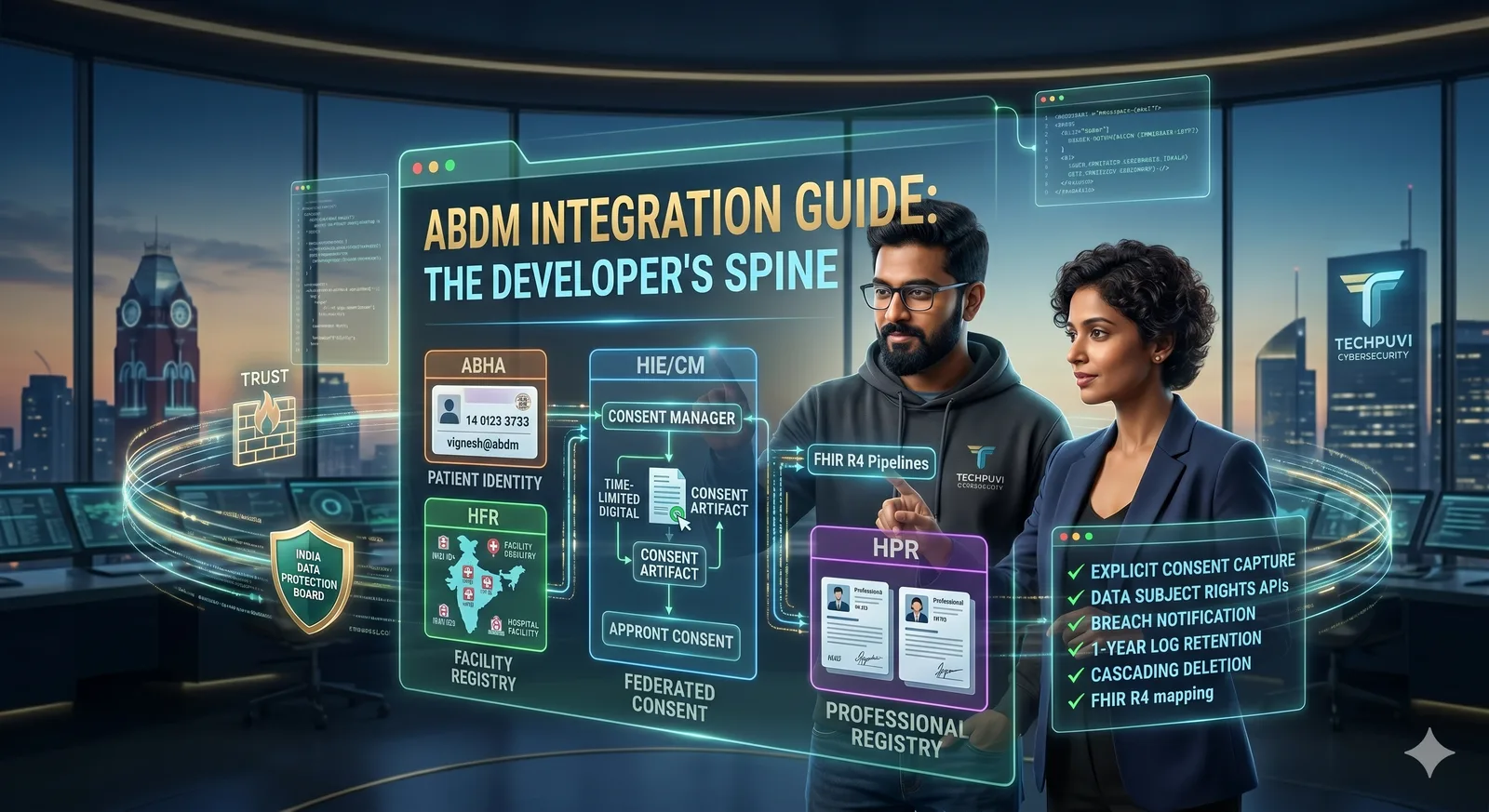
- ABHA is the patient's portable health ID, a 14-digit number plus an "abha-address" handle.
- HIE/CM is the Health Information Exchange and Consent Manager, where patients grant consent for one health system to fetch their data from another.
- HFR registers health facilities; HPR registers healthcare professionals. Both authenticate to ABDM.
- Architecturally, ABDM is a federated, consent-driven model. You don't store other people's patient data; you fetch it on-demand with consent, render it, and (usually) discard it.
- The hard parts are the consent UX, the FHIR mapping, and the testing sandbox edge cases.
Why this matters
Indian healthcare is fragmenting fast, telehealth, e-pharmacy, RPM, clinic chains, hospital networks, insurer-led primary care, and they all need to read and write the same patient record. ABDM is the standard that's actually being adopted. Building on it now is far cheaper than retrofitting later, and many government-linked programs require ABDM compliance as a procurement gate.
The four building blocks
ABHA (Ayushman Bharat Health Account)
Every Indian who opts in gets an ABHA number (14 digits) and an ABHA address (something like vignesh@abdm). Your app integrates an ABHA-creation flow (Aadhaar-based or mobile-OTP-based) and stores the patient's ABHA address linked to their profile.
HIE/CM (Health Information Exchange / Consent Manager)
The Consent Manager is where the patient's permissions live. When your app wants to fetch a patient's lab report from another health information provider (HIP), you initiate a consent request. The patient sees it in their ABDM app, approves it, and your app gets a time-limited consent artifact. You then exchange that artifact for the actual data.
HFR (Health Facility Registry)
Your hospital or clinic registers with HFR and gets a facility ID. This is the identity your app uses when acting as an HIP (Health Information Provider) or HIU (Health Information User).
HPR (Healthcare Professionals Registry)
Doctors, nurses, and other clinicians register with HPR. Their identity in the system is their HPR ID. When a clinician issues a prescription or makes a record, their HPR ID signs the action.
A typical end-to-end flow
A patient walks into your clinic. Receptionist asks for their ABHA address (or scans their ABHA QR). Your app verifies the address with the ABDM Gateway. The doctor wants to see the patient's prior lab reports from a different hospital. Your app initiates a consent request to HIE/CM, naming the data type (DiagnosticReport), the time range, and the purpose. The patient gets a notification in their ABDM app, approves it. Your app receives a consent artifact. With that artifact, your app calls the other hospital's FHIR endpoint, fetches the report, and renders it. After the consultation, your app uploads the new prescription and visit summary, signed by the clinician's HPR identity, and notifies the patient's ABDM record that new data is available.
That's the loop. Patient owns the data. Consent is explicit. Federation is real.
FHIR mapping
ABDM uses FHIR R4 with India-specific profiles. The common resources you'll encounter: Patient, Practitioner, Encounter, Observation, DiagnosticReport, MedicationRequest, Condition, Procedure. If you've worked with FHIR before, this part is familiar. If not, plan for a 2-3 week ramp.
The architecture pattern that works
Build an "ABDM adapter" service that sits between your core EHR/EMR and the ABDM Gateway. It handles consent state, retries, FHIR mapping, and audit logging. Your core app talks to the adapter via internal APIs; the adapter handles the ABDM-specific concerns. This insulates you from ABDM protocol changes (which happen).
Common pitfalls
The biggest one is treating ABDM as a one-shot API integration. It's a federation model with state machines, consent requests have lifecycles, can expire, be revoked, fail. Build for that.
The second is undertesting on the sandbox. The ABDM sandbox has edge cases the production system handles differently. Run end-to-end tests on the actual sandbox, and have a real ABHA-registered patient on your team for production smoke tests.
The third is forgetting audit. Every data access via ABDM must be logged. Build a structured audit log from day one.
What we recommend
Treat the first integration as a 6-10 week project. Allocate one engineer who reads the ABDM specs end-to-end. Use the sandbox heavily. Get your facility registered in HFR and a clinician identity in HPR before you write your first line of integration code, those steps take longer than they should.
FAQs
Do we need ABDM if we're a private telemedicine app? Not legally required for B2C, but increasingly expected by patients and required for any government-linked program.
Does ABDM store the patient's records? No. It indexes who holds what and orchestrates consent.
Can we cache fetched records? Subject to consent terms and your privacy policy, usually short-lived caching is acceptable, but document and disclose.
What about non-FHIR legacy systems? Build the adapter to translate. Plan for it.
See how Techpuvi builds for healthcare. ABDM-aware, FHIR-fluent, HIPAA-aligned where it counts.